It doesn’t sound pleasant to have glue in your ear, does it? Yet many children—and even some adults—live with a condition aptly named glue ear. The name is catchy, but the consequences are severe, particularly in terms of hearing, speech, and learning. In this guide, we’ll explore what glue ear is, why it happens, how it affects children, and what treatments are available.
Understanding glue ear
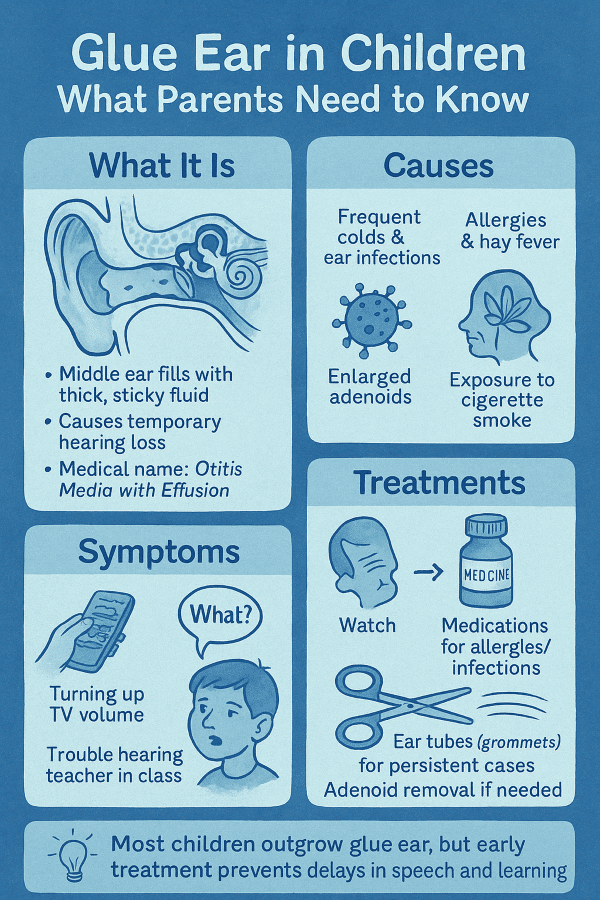
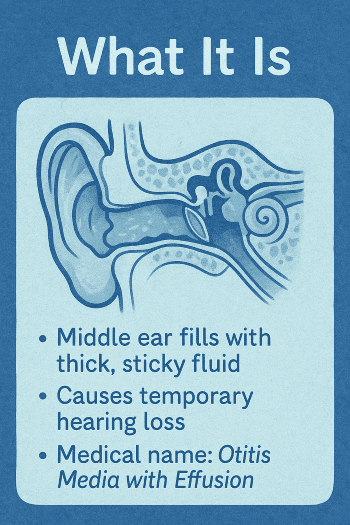
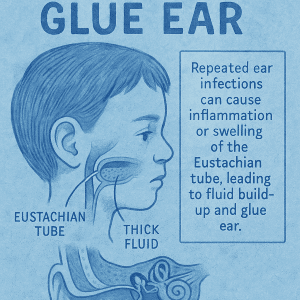
Glue ear is a condition where the middle ear fills with thick, sticky fluid that resembles glue. Normally, the middle ear is an air-filled space that allows sound waves to pass freely and the small bones inside—the ossicles—to move and transmit sound to the inner ear.
With glue ear, the presence of sticky fluid prevents those bones from moving correctly. As a result, sound is blocked or muffled, causing a temporary type of hearing loss known as conductive hearing loss.
Doctors refer to glue ear as otitis media with effusion (OME). Unlike a typical ear infection, glue ear typically does not involve sharp pain or fever. That’s why it can go unnoticed for weeks or months—until parents or teachers realize that a child isn’t hearing properly.
Glue ear is extremely common. Studies suggest that most children will have at least one episode of glue ear before the age of 10. Peak incidence occurs between the ages of 2 and 8, although babies, older children, and adults can also be affected.
Why does glue ear happen?
The culprit is usually a blocked or swollen Eustachian tube. This small canal connects the middle ear to the back of the throat, acting as a pressure valve. Its two main jobs are to:
- Equalize the air pressure in the ear
- Drain any fluid that builds up
.
In children, the Eustachian tube is shorter, more horizontal, and narrower than in adults. This makes it more prone to blockage. When it becomes inflamed—often due to a cold, sinus infection, or allergies—it stops functioning correctly. Fluid builds up in the middle ear, thickens over time, and becomes the sticky “glue” that gives the condition its name.
Risk factors for glue ear include:
- Frequent colds and respiratory infections – particularly common in young children at school or daycare
- Recurrent ear infections – children who’ve had several episodes of acute otitis media are more likely to develop glue ear
- Allergies and hay fever – which cause inflammation and swelling in the ear, nose, and throat
- Enlarged adenoids – soft tissue at the back of the throat that can block the Eustachian tube
- Exposure to cigarette smoke – secondhand smoke irritates the airways and increases the risk of middle ear problems
- Bottle-feeding while lying down – which can allow milk to enter the Eustachian tube more easily
- Seasonal factors – glue ear tends to be more common in the winter and spring when colds and flu circulate widely
Symptoms and signs of glue ear
The challenge with glue ear is that it often doesn’t hurt. Unlike acute ear infections, which usually bring pain and fever, glue ear can creep up quietly.
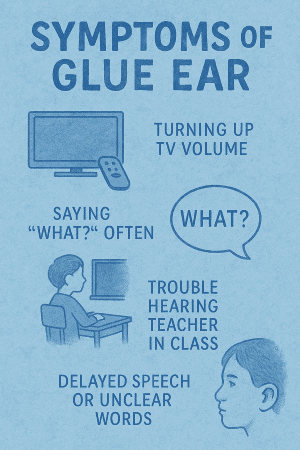
The most critical symptom is hearing loss. For parents and teachers, this often shows up as:
- A child turning up the TV or radio louder than usual
- Frequently saying “What?” or “Huh?” in conversations
- Trouble following instructions, especially in noisy classrooms
- Seeming distracted, inattentive, or daydreaming—when the real issue is that they can’t hear well
- Delayed or unclear speech in younger children
.
Some children also experience:
- A sense of fullness or pressure in the ear
- Mild, occasional earache
- Trouble with balance (since the ear plays a role in balance control)
- Behavioral changes, such as frustration or withdrawal
Because the hearing loss is often temporary but fluctuating, parents may think their child is ignoring them or being stubborn. In reality, the child may hear normally one day and then poorly the next, depending on changes in the fluid levels.
How does glue ear affect learning?
Hearing is critical during the early years of speech and language development. When children cannot hear well, they miss out on key sounds and words that shape vocabulary and pronunciation. This can lead to:
- Speech delays – difficulty pronouncing certain sounds or forming sentences
- Language delays – slower acquisition of new words and grammar
- Reading difficulties – since phonics and early literacy rely on hearing sounds clearly
- Classroom struggles – especially in noisy environments where a child with glue ear can’t pick out the teacher’s voice from background noise
Over time, untreated glue ear can also affect a child’s confidence and behavior. Frustration at not understanding instructions may be mistaken for inattention, hyperactivity, or laziness. Teachers might misinterpret the problem as a learning disorder when the root cause is temporary hearing loss.
How is glue ear diagnosed?
If a child shows signs of hearing difficulty, a visit to the doctor or an ear, nose, and throat (ENT) specialist is recommended. Diagnosis may involve:
- Otoscopy: Using a light to look at the eardrum. A retracted or dull eardrum may suggest fluid behind it.
- Tympanometry: A painless test that measures how the eardrum moves in response to slight air pressure changes. Lack of movement indicates fluid.
- Audiometry (hearing test): Helps determine the extent of hearing loss and categorizes it as mild, moderate, or more severe.
Some doctors may also use nasal endoscopy to check for enlarged adenoids if these are suspected to be contributing to blocked drainage.
Treatment options for glue ear
The best treatment depends on the severity, duration, and impact of the condition.
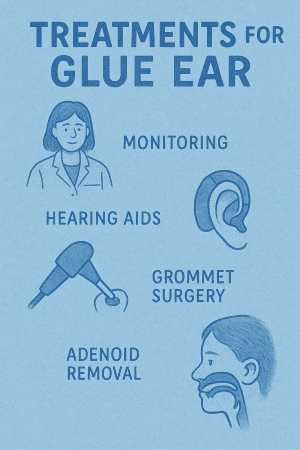
1. Watchful waiting
In many cases, glue ear clears up on its own within 6–12 weeks. Doctors often recommend monitoring hearing and symptoms for several months before intervening. This approach avoids unnecessary treatment, since about half of the cases resolve naturally within three months.
2. Medications
- Antibiotics may be prescribed if glue ear follows repeated infections, but they are not always effective against the fluid itself.
- Decongestants or antihistamines may help if allergies are involved, but they do not cure glue ear.
- Nasal steroids are sometimes tried for children with severe allergies or nasal inflammation.
.
3. Ear tubes (grommets)
For persistent glue ear—especially if it causes significant hearing loss or speech delays—ENT specialists may recommend inserting small ventilation tubes (grommets) into the eardrum. This quick surgical procedure allows fluid to drain and air to circulate in the middle ear.
Grommets usually stay in place for 6–12 months and often fall out naturally. Hearing typically improves immediately after the procedure.
4. Adenoidectomy
If enlarged adenoids are contributing to glue ear, doctors may recommend removing them during the same procedure as grommet insertion. This helps prevent recurrence.
5. Hearing aids
For children who cannot undergo surgery, temporary use of hearing aids may help ensure they don’t fall behind in language and learning while waiting for the glue ear to resolve.
Complications if left untreated
Most cases of glue ear are temporary. However, if left untreated for long periods, it can lead to:
- Persistent hearing loss
- Delayed speech and language development
- Academic struggles and learning difficulties
- Behavioral and social issues stemming from communication challenges
- Rarely, structural damage to the eardrum or middle ear bones
Can adults get glue ear?
Yes. While glue ear is most common in children, adults can also develop it, often after a bad cold, sinus infection, or allergies. In adults, persistent glue ear should always be evaluated carefully, as it may sometimes be linked to more serious underlying conditions (such as nasal growths blocking the Eustachian tube).
Helping a child with glue ear at home
While awaiting resolution or treatment, parents can help children cope by:
- Reducing background noise when speaking (e.g., turn off the TV during conversations)
- Getting the child’s attention before talking, so they can focus on lip-reading and facial cues
- Positioning the child near the front of the classroom to hear better
- Encouraging clear speech by repeating words gently and modeling correct pronunciation
- Monitoring progress in school and speech development closely, with teacher communication
The bottom line
Glue ear may sound like a minor issue, but its impact on hearing and learning can be significant. The condition is prevalent in children, usually temporary, and in many cases clears on its own. Still, because hearing is essential for speech and academic development, persistent glue ear should never be ignored.
With proper diagnosis and treatment—whether through careful monitoring, medication, or minor surgery—most children with glue ear recover fully and go on to hear, speak, and learn without difficulty.
This article is for educational purposes only and is not a substitute for professional medical advice. Always consult your healthcare provider for any health-related concerns.